The AI War Inside Your Hospital Bill

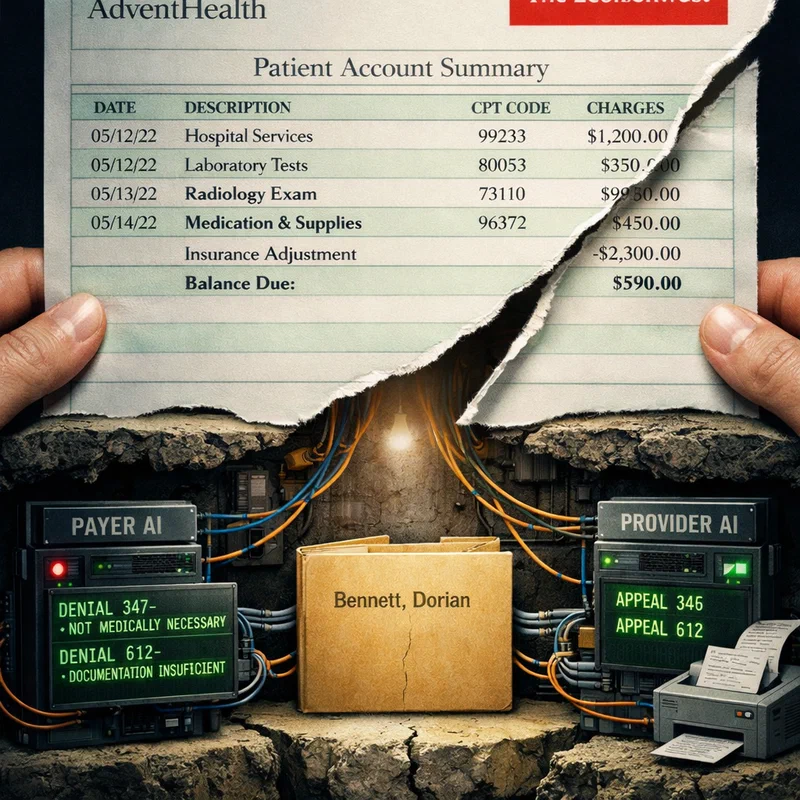
In November 2020, Bisi Bennett went into labor at seven months pregnant. Halfway to AdventHealth hospital, with her husband Chris behind the wheel, she gave birth to their son Dorian in their Mitsubishi Outlander. He didn’t breathe. At the hospital, she heard four words she will never forget: “We’ve got a pulse.” Dorian spent 56 days in the neonatal intensive care unit. He survived. The Bennetts then spent months fighting with their insurance company over whether the NICU stay was medically necessary — a battle adjudicated, in part, by algorithms neither side had fully seen.
This is the healthcare AI story that is not making headlines. And it may be the most important one.
The invisible arms race #
On June 3, 2026, STAT News published what should have been a front-page story: “The medical-billing AI arms race between providers and insurance: Both sides are training algorithms to fight over the same patient record.” Written by Dr. Darshak Sanghavi, a pediatric cardiologist and former senior federal health official, the piece documented something most patients never see — that artificial intelligence is now the primary combatant on both sides of every disputed medical claim.
The contours are stark. Health insurers deploy AI systems trained to flag claims for denial — identifying billing codes that exceed algorithmic thresholds, patterns that deviate from automated coverage rules, documentation gaps that a machine can reject faster than any human adjuster. Meanwhile, hospital revenue cycle teams deploy their own AI to pre-emptively optimize claims for approval and automatically generate appeals when denials arrive. The same patient record is processed by two AI systems with opposing incentives. The patient is not a participant in either system.
The consequences are measurable. In May 2026, Congressional Democrats introduced resolutions to overturn the Wasteful and Inappropriate Service Reduction (WISeR) program — a Medicare pilot using AI to authorize or deny care for seniors across six states. The GAO ruled the program should have been submitted for congressional approval before its January launch. Senator Ron Wyden (D-Ore.) stated: “The last thing seniors need is even more AI denying the care they need.”
The WISeR pilot was designed as an efficiency measure — AI streamlining prior authorization, cutting waste. But once deployed, the algorithm’s logic for approving or denying care became a black box that neither patients nor their physicians could interrogate. That is the structural risk that no pilot evaluation anticipated.
When the algorithm denies, who appeals? #
The same week, the American Medical Association joined lawmakers in a coordinated pushback against AI-driven care denials, as Mario Aguilar reported for STAT. The AMA represents physicians increasingly unable to explain denials to patients — because the reasoning resides in a model they cannot inspect.
This matters for a reason that extends beyond billing. Trust in clinical AI depends on a foundation of transparency and accountability. When AI systems deny care — not recommend, not flag, but deny — and patients cannot appeal to a human who understands the system’s reasoning, the damage accumulates against every other AI application in healthcare. A patient whose chemotherapy prior authorization was rejected by an opaque algorithm will not trust the AI system that triages their next emergency department visit, or the ambient scribe that documents their next consultation.
Brittany Trang’s AI Prognosis coverage at STAT has documented this tension. At Stanford Health Care, patient panels reviewing AI tools consistently raised concerns about control — who decides, who audits, who intervenes. The Stanford panel process, led by the HEAL-AI Lab, exposed “fault lines”: patients and hospitals disagree on foundational AI governance questions, and neither side has acknowledged the depth of the divide.
The data quality problem beneath the AI #
The billing AI arms race has a hidden weakness: garbage in, gospel out. Both sides’ algorithms depend on the same clinical documentation. If that documentation contains errors or ambiguities — which it frequently does — the AI systems amplify those flaws.
Trang documented this in her June 10 newsletter with a pointed headline: “Your sepsis algorithm shouldn’t require a time machine.” The issue she identified was that sepsis detection algorithms at multiple hospitals were generating inconsistent predictions because the underlying data — timestamps, vital sign measurements, lab values — were captured with varying precision across different EHR systems. An algorithm that works in one hospital’s data environment fails in another’s, not because the model is worse, but because the data plumbing is different.
Now apply that same logic to billing AI. If a physician’s note uses ambiguous language or a coder selects the wrong billing code, the insurer’s denial AI will reject the claim — and the hospital’s appeal AI will generate an automated rebuttal based on the same flawed documentation. Both algorithms are correct within their operational parameters. Neither produces a just outcome.
This is the paradox Sanghavi identified in the June 3 STAT piece: “The most consequential deployment of artificial intelligence in American health care is in medical billing.” The systems are deployed, they are scaling, and they are making decisions with direct financial and health consequences — on top of a data foundation that no one would consider adequate for clinical decision-making.
The market is voting with capital #
While billing AI proliferates in relative obscurity, the visible healthcare AI market is sending a different signal — one that reinforces the same structural problems.
Roche’s acquisition of PathAI for $750 million upfront (plus up to $300 million in milestones) signals confidence in AI-powered pathology. OpenEvidence, the AI chatbot for clinicians, claims 650,000 active U.S. physician users and a $12 billion valuation. These are genuine innovations with real potential. But both operate in the diagnostic and clinical decision support space — where AI’s errors are visible, reviewable, and subject to regulatory oversight through the FDA’s 510(k) clearance pathway.
Billing AI operates in a regulatory blind spot. The FDA’s framework for AI/ML-enabled medical devices, which Trang critiqued in May for allowing many AI devices to reach market through less rigorous clearance pathways, does not even extend to administrative AI systems that determine coverage. These systems are not medical devices. They are financial optimization tools. And they are reshaping access to care without any of the transparency, validation, or monitoring requirements we apply to a pulse oximeter.
An AI that helps a radiologist detect a lung nodule requires FDA clearance, validation studies, and post-market surveillance. An AI that denies the prior authorization for that same CT scan requires none of those things.
Separating the trust problem from the technology problem #
The billing AI crisis is not fundamentally a technology problem. The algorithms work as designed — they deny claims that match their training data’s pattern of “not medically necessary,” and they generate appeals that maximize expected reimbursement. The technology functions. The problem is the structural incentive: deploying AI in an adversarial relationship between two parties (insurer and provider) with a third non-participating party (the patient). The insurer’s AI is optimized to minimize payout. The provider’s AI is optimized to maximize reimbursement. Neither is optimized for accuracy, fairness, or clinical appropriateness.
If these algorithms were deployed in a clinical trial for a new drug, institutional review boards would flag the lack of a patient-centered endpoint. In the billing context, no equivalent oversight exists.
What would change this? #
Three shifts could alter the trajectory.
First, transparency requirements for utilization management AI. If an AI system participates in a coverage decision, the logic of that decision should be auditable — not necessarily interpretable by a layperson, but reviewable by a qualified clinician or regulator. The GAO finding that WISeR required congressional approval establishes the principle that algorithmic coverage decisions are policy decisions, not technical ones.
Second, payment model reform that aligns incentives. The current fee-for-service structure creates the adversarial dynamic that billing AI exploits. Prospective payment, bundled payments, and capitation models reduce the incentive to fight over individual claims. They do not eliminate the need for oversight, but they change the AI’s objective function from “win the denial/appeal battle” to “manage appropriate utilization.”
Third, patient representation in AI governance. The Stanford patient panel model should not be exceptional. Every health system deploying AI — whether clinical or administrative — should include patients in the governance structure. The HEAL-AI Lab’s work at Stanford demonstrates that patients consistently identify concerns that clinical and technical teams miss: about notification, consent, the right to opt out, and the meaning of algorithmic recommendations in their specific context.
The uncomfortable truth #
On May 27, 2026, Brittany Trang quoted a Defector article in her AI Prognosis newsletter that captured a sentiment most healthcare AI reporting dances around: “Wow! America’s Graduating Seniors Really F—ing Hate AI!” The piece documented the extent of AI skepticism among young adults — not Luddite resistance, but a specific, informed distrust of systems that make consequential decisions without transparency or recourse.
That distrust is rational. It is shaped by experiences like the one Bisi Bennett had — fighting an invisible adjudicator over whether her son’s NICU stay was necessary. And it is a warning: if we allow the billing AI arms race to continue without oversight, the window of trust for clinical AI — the diagnostic systems, the drug discovery platforms, the ambient scribes that could genuinely improve care — will close before those technologies reach the patients who need them most.
The AI war inside your hospital bill is not a skirmish in a corner of the healthcare system. It is the front line where trust in medical AI will be won or lost. The algorithms are already deployed. The question is whether the rest of us will catch up before the Bennetts of this world lose their faith entirely.
References #
- Sanghavi, D. (June 3, 2026). “The medical-billing AI arms race between providers and insurance.” STAT News. https://www.statnews.com/2026/06/03/ai-arms-race-medical-building-waste/ (Accessed June 16, 2026)
- Aguilar, M. (June 11, 2026). “AMA and lawmakers push back on AI care denials.” STAT News. https://www.statnews.com/2026/06/11/ama-lawmakers-push-back-ai-care-denials-health-tech/ (Accessed June 16, 2026)
- Trang, B. (May 20, 2026). “Congressional Democrats try to force a vote to end Medicare AI prior authorization pilot.” STAT News. https://www.statnews.com/2026/05/20/democrats-force-vote-to-end-medicare-ai-prior-authorization-pilot/ (Accessed June 16, 2026)
- Trang, B. (May 27, 2026). “Where patients and hospitals disagree about AI.” STAT News. https://www.statnews.com/2026/05/27/health-ai-where-patients-hospitals-disagree-ai-prognosis/ (Accessed June 16, 2026)
- Trang, B. (May 27, 2026). “How Stanford patients help expose ‘fault lines’ in health AI adoption.” STAT News. https://www.statnews.com/2026/05/27/stanford-patient-panels-feedback-on-ai-shaping-health-care/ (Accessed June 16, 2026)
- Trang, B. (June 10, 2026). “Your sepsis algorithm shouldn’t require a time machine.” STAT News. https://www.statnews.com/2026/06/10/sepsis-algorithm-shouldnt-require-time-machine-ai-prognosis/ (Accessed June 16, 2026)
- Trang, B. (May 13, 2026). “AI medical devices’ dirty FDA secret.” STAT News. https://www.statnews.com/2026/05/13/ai-medical-devices-dirty-fda-secret-ai-prognosis/ (Accessed June 16, 2026)
- Saltzman, J. — Boston Globe (May 8, 2026). “Roche to buy PathAI for $750 million.” STAT News. https://www.statnews.com/2026/05/08/roche-acquire-startup-pathai-750-million-upfront/ (Accessed June 16, 2026)
- Palmer, K. (May 20, 2026). “OpenEvidence makes its pitch to hospitals. ‘We’re not crazy monsters.’” STAT News. https://www.statnews.com/2026/05/20/openevidence-pitches-hospitals-we-are-not-monsters/ (Accessed June 16, 2026)
- Wyden, R. et al. (May 20, 2026). “Murray, Wyden, Gillibrand Lead Democrats in New Bill to Halt Trump Administration’s Looming Medicare AI Prior Authorization Takeover.” https://www.murray.senate.gov/murray-wyden-gillibrand-lead-democrats-in-new-bill-to-halt-trump-administrations-looming-medicare-ai-prior-authorization-takeover-democrats-fight-to-save-medicare/ (Accessed June 16, 2026)
- Senate Finance Committee (May 20, 2026). “WISeR CRA Resolution.” https://www.finance.senate.gov/imo/media/doc/052026_wiser_cra_resolution.pdf (Accessed June 16, 2026)
AI Content Notice
This article was created using artificial intelligence technology. Whenever possible, we include references and sources to support the information presented. Readers are encouraged to consult these sources for further information. While we strive for accuracy and provide valuable insights, readers should independently verify information and use their own judgment when making business decisions. The content may not reflect real-time market conditions or personal circumstances.
Related Articles
AI Can Now Outdiagnose Doctors. That's the Easy Part.
This week’s clinical AI milestones reveal a structural fault line: the capability to transform …
The Slide That Could Save Everyone — If the Model Works for Everyone
The AACR 2026 AI pathology revolution promises to turn penny-cheap H&E slides into precision …
Ambient AI's Fastest Win Is Also Healthcare's Next Infrastructure Test
Ambient AI scribes are not creating a winner-take-all model race in healthcare; they are creating a …